Effects of Myofascial Release on Human Performance

The Study
Considering the number of people who participate in fitness and athletic activities there needs to be a better understanding of what needs to be done before activity to improve performance and assure injury prevention. One warm up activity and rehabilitation technique that seems to have a great deal of following is myofascial (muscular) releasing. Myofascial releasing is a therapeutic self-massage technique where body weight is applied to specific areas by rolling on a round foam roller or soft balls. Self-myofascial release techniques have been suggested to improve flexibility, function, and performance and reduce the chance of injuries. After a search of the literature there seems to be no scientific research that has investigated the effects of self muscle releasing on range of motion, strength, power, and perceived function. Identifying a relationship between myofascial release and a battery of performance measures would help those utilizing the technique in the field establish a research base for their practical applications. It would also help add to the body of knowledge regarding warm-ups for physical activity, optimal preparation for athletic competition, and the effects of massage on human performance.
Methods
Participants:
In a repeated measures experimental design thirteen strength trained subjects will perform two training techniques to their hamstring musculature. Subjects will be selected based on accessibility for testing, the only other qualifying characteristic is at least 6 recent months of strength training. Subjects will be an assortment of personal trainers and clients from two separate personal training studios. The data collection will involve 3 meetings between subject and tester, spanning 3 to 4 weeks. Therefore, the subject’s ability to participate in the testing on a somewhat rigid schedule without any planned conflicts will be an important consideration. Subjects will not be selected based on age or sex. Prior to participation subjects will be required to sign an informed consent form detailing the purpose of the study and their rights during the experimental process. A form will be submitted to the Institutional Review Board of Bridgewater State College for approval of research using human subjects. Once a group of thirteen subjects has been established and informed consent forms are signed and collected, the testing will begin.
A repeated measures design will have the subjects participating in both the control and treatments groups. Standard stretching and muscular releasing will be the training techniques. Subjects will be equally divided into 2 groups. Grouping is being employed to control for a training effect. Group one will perform standard stretching first and after 2 weeks or more of recovery subjects will perform muscular releasing to their right leg, while group two will perform muscular releasing first and standard stretching after 2 or more weeks of recovery.
Criterion measures will be recorded on the right leg on two separate occasions before treatments. This data will act as the control and be used to determine the reliability of the criterion measures.
Procedures:
Criterion Measures
1. Strength
Isometric strength of the knee flexors will be taken before and after the performance of each training technique. Subject's isometric knee flexor strength will be measured at the joint angle of 90 degrees in the prone position with test ankle flexed to 90 degrees. A cuff will be attached to the ankle. A chain will be attached to the cuff and to a dynamometer via a clip or hook. The chain will be kept parallel to the floor while the subject exerts a maximal isometric action by flexing the knee while the examiner is holding onto the dynamometer keeping chain parallel to floor. The thigh of the both legs must remain in contact with floor to avoid use of other muscles. Each isometric action will be held for 5 seconds followed by 1 minute recovery. Peak values will be recorded and the mean of the 3 trials will be taken as the criterion score.
2. Range of motion
Range of motion will be assessed using two protocols:
Supine range of motion of the hamstring muscle will be taken before and after the training technique. The subject will take a supine position, with the non-test leg against the floor. The tester will take the subject's leg into hip flexion while keeping the test leg’s knee extended until the first resistance barrier and/or any spinal motion. The non-test leg will remain in contact with the floor and the test legs foot will be dorsiflexed to 90 degrees. No forced stretches will be made. The leg will only be taken to the point of first resistance barrier. At this point the perpendicular distance from the heel to the floor will be measured in millimeters and the distance will be recorded. The test leg must remain in its stretched position when measuring.
Seated range of motion of the hamstring muscle will be taken after the supine range of motion measure. Seated hamstring range of motion will be determined by having the subject seated in a figure 4 position with test leg straight with foot dorsiflexed to 90 degrees and non-test leg's foot's plantar aspect touching the medial knee aspect of test leg. The non-test leg is in a relaxed abducted position. The subject will reach as far forward with both hands until the first resistance barrier is met. No bouncing or forced stretch should be made. One hand will be placed on top of the other with palms facing down. The distance between index fingers and top of test foot will be recorded in millimeters where the top of test foot is considered zero and the distance reached before foot is recorded as a negative value and beyond as a positive value.
3. One leg jump
One leg jump performance measures will be taken before and after the training technique. Subjects will stand on one leg and will jump forward as far as they can.
Subjects will be advised to land on both feet in order to avoid injury. The subjects will
be allowed to squat down with test leg and to use both arms in the jumping motion. The non-test leg should be bent and will not be allowed to touch the ground until landing. Distance in millimeters will be recorded as the starting point to the heel of test foot at landing. Three trials will be followed by a 1 minute recovery. Peak values will be recorded and the mean of the 3 trials will be taken as the criterion score.
The training techniques
Stretching
Stretching treatment will resemble seated range of motion criterion measure. Subject will be seated in a figure 4 position with test leg straight with foot dorsiflexed to 90 degrees and non-test leg's foot's plantar aspect touching the medial knee aspect of test leg. The non-test leg is in a relaxed abducted position. The subject will reach as far forward with both hands until the first resistance barrier is met. No bouncing or forced stretch should be made. One hand will be placed on top of the other with palms facing down. When full resistance barrier is met the stretch should be held for 30 seconds. Thereafter the subject should rest for 10 seconds and the technique is repeated two more times. The ROM criterion measure will be taken immediately after stretching. After ROM measures strength measures will be assessed. After measuring strength the subject will perform the one leg jump test. After one leg jump measures are recorded stretching treatment and subsequent testing will be completed.
Self-Muscular releasing on the floor
The subject will sit down on the floor placing a 6 inch foam roller underneath their hamstrings perpendicular to the body, closer to the back of the knee. The upper body of the subject should make close to a 90 degree angle with the lower body. The leg of the test leg should be extended and the foot should be dorsiflexed to 90 degrees pointing straight upwards. The non-test leg should be bent where the foot is flat on the floor. The subject should place their hands beside their hips behind the roller and they should push up elevating their body from the floor slightly shifting to the side of the test leg. This places pressure on the test leg’s hamstring. While muscular releasing the subject should bend forward from the waist until the first resistance barrier. When first resistance barrier is met the subject should roll along the roller so that he or she moves on top of the roller, from knee (hamstring insertion) to buttock (hamstring origin), and then the motion is reversed from buttock to knee. The subject’s full weight should be applied to the roller. This forward and backward motion theoretically creates a releasing effect. Each motion will be done to a 3 count where 15 back and forth motions should be made which should take roughly 90 seconds. This treatment should not exceed 90 seconds. The ROM criterion measure will be taken immediately after releasing. ROM will be recorded after range of motion measures. After taking ROM measures strength will be assessed. After measuring strength the subject will perform the one leg jump test. After one leg jump measures are recorded muscular releasing treatment and subsequent testing will be completed.
Statistical Analysis
Criterion measures will be analyzed by determining the difference between baseline and treatment measures for the groups (releasing and stretching), followed by a t test to determine any significant changes between the two treatments. To determine the reliability of range of motion, isometric strength, and one leg jump, baseline values will be recorded on two days. The criterion for statistical significance was set at p < 0.05.
Results
Range of motion
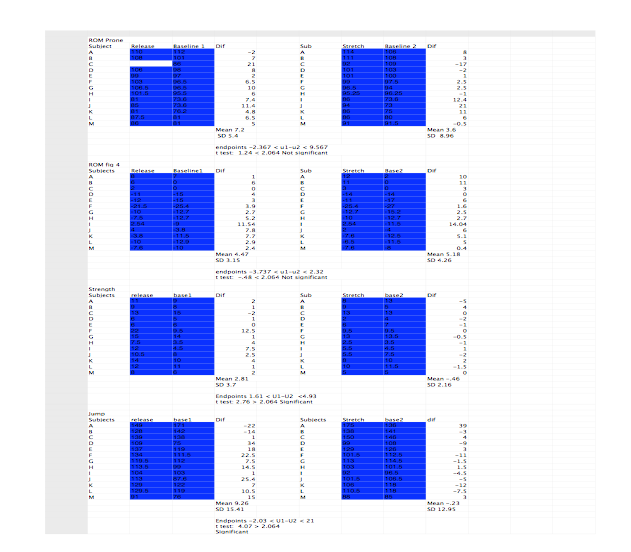
No significant changes were found between SMR and SS for either ROM measure. For the prone ROM measure, the difference between the baseline and treatment for SMR was a mean of 7.2 centimeters with a standard deviation of 5.4. The difference between the baseline and treatment for SS was a mean of 3.6 with a standard deviation of 8.96. For the figure-4 ROM measure, the difference between the baseline and treatment for SMR was a mean of 4.47 with a standard deviation of 3.15. The difference between the baseline and treatment for SMR was a mean of 5.18 with a standard deviation of 4.26. Neither of these differences between treatments reached significance. A T-test for the prone ROM measure yielded 1.24, compared to a 2.064 needed to identify a significant difference. A t-test for the figure 4 ROM measure yielded -.48, compared to a 2.064 needed to identify a significant difference. In summary, no significant differences were found between SMR and SS in the two ROM measures of the hamstring musculature.
Strength
A significant difference was found in isometric strength measures when SMR was compared to SS. The difference between the baseline and treatment for SMR was a mean of 2.81 with a standard deviation of 3.7. The difference between the baseline and treatment for SS was a -.46 with a standard deviation of 2.16. The difference between these two reached significance. A t-test for the strength measure yielded 2.76, exceeding the 2.064 needed to identify a significant difference. In summary, a significant difference existed between SMR and SS in the strength measure of the hamstring musculature.
One leg jump
A significant difference was found in one leg jump measures when SMR was compared to SS. The difference between the baseline and treatment for SMR was a mean of 9.26 with a standard deviation of 15.41. The difference between the baseline and treatment for SS was a mean of -.23 with a standard deviation of 12.95. The difference between these two reached significance. A t-test for the one leg jump measure yielded 4.07, exceeding the 2.064 needed to identify a significant difference. In summary, a significant difference existed between SMR and SS in the one leg jump measure of the hamstring musculature.
Discussion
The purpose of this investigation was to provide insight into the tangible value for self myofascial releasing rollers, especially compared to static stretching. While there is growing anecdotal evidence of self myofascial release’s efficacy, to date there are no formal studies that have been performed to measure it’s effects. Generally speaking, the value of a pre-exercise warm-up is not questioned. If for no other reason, the perceived feelings of well being and improved physical capacity make warming up before any physical activity a helpful endeavor. In terms of human performance however, practicality and efficacy take precedence. Doing something simply because it “feels good” is not enough of an incentive for a high level athlete and his or her strength and conditioning. Quantifiable evidence needs to exist that the method being utilized is effective. This is where this particular study and ultimately further research should help shed light on the value of SMR.
ROM was greater in both SS and SMR treatments when compared to the control, where there was no difference between conditions. SS is generally a recommended method for increasing ROM as it has been found to be effective, safe, and easy to implement. In light of the findings of this study, SMR may be used in addition to or in replacement of SS. The increase in ROM from SMR may be due to the focal lengthening that the musculature experiences when the roller is contacting the muscle while under body weight pressure. A stretch also occurs to the hamstring and gluteal musculature from body positioning while performing releasing to the hamstring musculature.
SMR was shown to increase static strength of the hamstring musculature. This is the first study to show this effect. Research investigating massage has thus far been inconclusive at affecting strength. SMR producing an increase in strength may be due to a warm up effect of the musculature that massage does not offer. SMR of the hamstring musculature requires the arms to prop up the upper body and move the extended leg along the roller with the aid of the opposite leg, such an action requires an increase in total body metabolism. Studies have shown that a warm up activity which raises metabolism, like dynamic stretching, tends to in increase strength. SS was shown not to affect strength. This is interesting considering that some studies show a strength loss with SS. This study used recreationally weight trained subjects. Subjects in studies that were trained did not generally show a strength loss after SS. The results presented confirm the results of these SS studies.
JUMP was increased with SMR compared to the control as well. Significance was reached despite the investigators suspicion that one subject may have been attempting to corrupt the data with an awareness of the hypothesis for personal reasons. Had this subject been omitted from the data, the data would have shown even greater significance. The increase in jump performance may be attributed to the same mechanisms suggested for the increase in strength. This improvement with SMR compared to SS suggests that the improvements sought after with a warm-up are not limited to isometric strength but unilateral power as well.
Given the results of this study, SMR should be considered as a valuable tool for preparing a competitive or recreational athlete for exercise. Based on the data collected, it appears SMR offers increased strength and jumping ability, without any difference in transient ROM improvements that SS is perceived to offer. The method can be implemented immediately preceding any type of resistance, plyometric, or speed training session. Based on the current research, a combination of myofascial release, dynamic stretching, and specific low load muscle activation could be an ideal warm-up protocol for any type of workout. Given the obvious narrow scope of this study, focusing exclusively on the hamstring musculature, it may be premature to anoint SMR as an appropriate and effective technique for any and all athletes. More research is needed using alternative protocols, different fitness tests, and alternative muscle groups. However, with mounting anecdotal evidence in favor of SMR and now a small amount of research demonstrating efficacy, fitness professionals would be well served to familiarize themselves with various SMR techniques.
By Anthony D’Amico
and
Christopher Morin
in association with Bridgewater State University
Abstract
Myofascial releasing rollers are muscle massage devices used by athletes, fitness enthusiasts, and those recovering from injury to enhance functional ability. OBJECTIVES: The purpose of this study was to assess the acute effects of self myofascial releasing rollers on muscle strength, power, and flexibility compared to static stretching and control. STUDY DESIGN: Thirteen adult recreationally trained subjects consented to participate in a 3-week, counterbalanced repeated measure study, which consisted of 3 testing sessions (1 baseline and 2 data collection) scheduled 2 weeks apart. METHODS: Criterion measures of range of motion (ROM) of the hamstring musculature both seated and supine, isometric strength of the knee flexors (STR), and one leg jump power test (JUMP) were measured at one week before treatment conditions (baseline 1), before treatment conditions (baseline 2), and after treatment conditions of self-myofascial releasing (SMR) and static stretching (SS). Baseline 1 and 2 acted as the control (CONT). Statistical analyses involved a t test determining significant differences in treatments. RESULTS: There was no significant difference between SMR and SS in ROM. There was a significant difference between SMR and SS in STR. There was also a significant difference between SMR in JUMP. CONCLUSIONS: SMR increases ROM as much as SS. SMR increases isometric strength and increases jumping ability compared to SS and a control. IMPLICATIONS: SMR can improve acute ROM and may be used with or in replacement of SS towards improving ROM. SMR may be used as an aid before strength or power performance.

New Important Research Study in association with FitTec
Click Here for Complete Study
including a Review of Literature
Click Here for Complete all data